- Have any questions?
- 480-631-7837
- support@in-goodhealth.com


Thyroid Self-Exam: How to Check Your Thyroid at Home in Two Minutes
March 10, 2026
Carbohydrate Timing and Cortisol: Why Evening Carbs May Improve Sleep and Energy
March 24, 2026Thyroid Self-Exam: How to Check Your Thyroid at Home in Two Minutes
March 10, 2026Carbohydrate Timing and Cortisol: Why Evening Carbs May Improve Sleep and Energy
March 24, 2026
If you’ve been “doing everything right”: taking your meds, cleaning up your diet, and tracking your labs, yet you still struggle with unstable thyroid levels or crashing fatigue, the problem might not be your thyroid at all. It might be your stomach.
There is a frequent, yet often silent, partner to Hashimoto’s disease called Autoimmune Gastritis (or Thyrogastric Syndrome). Recent estimates suggest that as many as 30% to 40% of people with Hashimoto’s are also dealing with this condition, often without realizing it until a major nutrient deficiency takes hold.
Recommended Product: RS Complete is a clean, reliable way to get a precise daily dose of Type II resistant starch—without excess carbs, kitchen prep, or guesswork. Each scoop delivers 4 grams of standardized RS from high-quality plant sources, formulated to be gentle on sensitive guts. Click Here
Table of Contents
The "Cluster" Effect
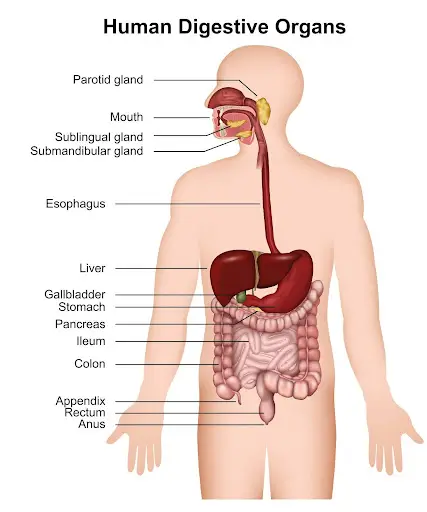
Autoimmune conditions rarely travel alone. When your immune system is primed to attack your thyroid proteins, the “misfire” can easily spread to other organs. In the case of Thyrogastric Syndrome, the immune system sets its sights on your stomach’s parietal cells.
Why does this matter for your thyroid? Parietal cells are the “gatekeepers” of your nutrition. They are responsible for producing two vital substances:
- Hydrochloric Acid (HCl): Necessary for breaking down protein and absorbing iron.
- Intrinsic Factor: The essential “key” required to absorb Vitamin B12.
When these cells are under attack, your body loses its ability to move iron and B12 from your food (or even your supplements) into your bloodstream. If your stomach can’t process these nutrients, your thyroid can’t function properly—no matter how many pills you take.
How Autoimmune Gastritis Works: The Digestive And Nutritional Cascade
The parietal cells in the stomach have two central roles. First, they secrete hydrochloric acid, or HCl, which helps break down proteins, ionize minerals like iron and zinc, and set the stage for digestion. Second, they produce intrinsic factor which chemically modifies vitamin B12 so it becomes absorbable. When autoimmune gastritis attacks parietal cells, both HCl production and intrinsic factor fall. The result is a twofold problem: low stomach acid and poor B12 absorption.
There is a less obvious but equally important factor: mucin production. The same stomach lining that regulates acid also secretes mucin, a protective, viscous layer that shields the stomach from its own acid. Mucin production falls along with HCl when parietal cells are affected. That loss of mucin means the stomach cannot tolerate added acid the same way it used to. This interplay is why the common functional medicine reflex, simply adding HCl pills for low stomach acid, can be short-sighted or even risky in the context of autoimmune gastritis.
Symptoms To Watch For: Digestive Clues And Nutrient Deficiency Signs
Autoimmune gastritis often begins subtly. Early symptoms may be vague or absent, and yet nutrient deficiencies can be quietly developing. Digestive signs include early post-meal bloating, upper abdominal gas, unexplained heartburn, or marked fatigue after heavy, protein-rich meals. You might notice that a big protein dinner leaves you wiped out and sleepy in a way that feels different from ordinary fullness.
Systemic symptoms tend to come from malabsorption. Iron deficiency is often the first nutrient to be affected. Women are more frequently symptomatic because regular menstrual blood loss makes iron depletion easier to tip into deficiency. Low iron commonly manifests as tiredness, foggy thinking, mood shifts, and specific hair thinning.
As damage advances, B12 deficiency symptoms appear. Vitamin B12 deficiency causes macrocytic changes to red blood cells and can damage peripheral nerves. Numbness or tingling in hands and feet, burning or electric-like sensations, balance problems, forgetfulness, and heightened anxiety or stress responses can all be signs of low B12. When B12 is low enough for neurological symptoms, timely diagnosis and treatment become urgent to prevent permanent nerve damage.
Further progression can affect zinc and calcium handling, undermining bone health, skin repair, and hormone balance. Because autoimmune gastritis can present with digestive symptoms in roughly two-thirds of cases, up to a third of people have no overt digestive complaints but still carry the condition. That makes proactive screening important for anyone with Hashimoto’s disease who has unusual fatigue, cognitive changes, hair loss, or unexplained lab abnormalities.
Why “Low Stomach Acid” Is Only Part Of The Story
“Low stomach acid” is a common phrase in natural thyroid solutions, and it often points people toward hydrochloric acid supplements. There are circumstances where supplemental HCl helps short term. However, in autoimmune gastritis the problem is not just low HCl; it is a loss of the entire protective system–intrinsic factor and mucin production included. Adding acid back in without addressing mucin may irritate an unprotected stomach lining and fails to correct intrinsic factor loss, so B12 absorption will still lag.
There is also an important long-term risk to consider. Chronic, untreated autoimmune gastritis increases the risk of stomach and esophageal cancers. When gastritis has advanced, some diagnoses are only made after serious complications arise. That makes careful evaluation and close follow-up more than academic: it can be lifesaving. This is why a reflexive recommendation to “take HCl” is not the best blanket approach in people with autoimmune thyroid disease and suspected thyrogastric syndrome.
––Key takeaway:. Reflexive HCl supplementation is short-sighted, fails to correct B12 malabsorption, and is risky.
How To Know If Autoimmune Gastritis Is Present: The Testing Pathway
If you have Hashimoto’s disease and symptoms or lab findings that point toward malabsorption, the next step is screening. The first blood test to ask about is the antiparietal cell antibody test, commonly abbreviated as the APCA test. A positive APCA is a strong early indicator that autoimmune gastritis is occurring. False positives are uncommon, so a positive APCA is meaningful and should trigger closer attention.
The second useful blood marker is gastrin. Elevated gastrin levels often indicate that the stomach lining is being damaged and parietal cell function is reduced. Gastrin tends to rise as a compensatory response when acid is low and the body attempts to stimulate more acid production. A normal gastrin with a positive APCA suggests autoimmunity is present but significant mucosal damage has not yet occurred, which is a window where early intervention can make a difference.
If gastrin is elevated, that typically prompts consultation with a gastroenterologist and consideration of an upper endoscopy. Endoscopy visualizes the stomach and esophagus directly and allows biopsies. Given the increased cancer risk when gastritis is advanced, endoscopic surveillance is appropriate if gastrin or symptoms suggest significant mucosal damage.
Beyond APCA and gastrin, you should check nutrient status comprehensively. A full iron panel including ferritin is essential because ferritin typically drops early. Check vitamin B12 and consider methylmalonic acid if B12 is borderline. Zinc and vitamin D measurements can be helpful as well, and tracking these values over time gives a roadmap for intervention. Also be mindful that this process can interfere with absorption of thyroid medications; in some cases switching to a liquid or gel cap form of levothyroxine or desiccated thyroid can improve reliability.
Treatment Principles: Protect, Restore, And Replace Where Needed
Managing autoimmune gastritis combines several goals: minimize ongoing immune-mediated damage where possible, protect the stomach lining, support digestion without doing harm, and replace deficient nutrients effectively.
Protecting mucin production is central. Rather than simply adding HCl, support the stomach’s protective mucus layer by using mucilaginous foods. Cabbage is one of the most effective options. Juiced cabbage (blended with apple or other vegetables for flavor), slow-cooked cabbage soups, and regular inclusion of cabbage in meals are practical and evidence-informed ways to support mucin. Okra and certain squashes also have mucilage and can soothe the lining. These foods are inexpensive, accessible, and, importantly, they address the mucin production aspect that HCl pills do not.
Improving digestive enzyme activity helps you do better with less acid. Culinary herbs and spices like ginger, garlic, turmeric, and cumin stimulate enzyme production and improve digestion. Bitter greens such as arugula, kale, and dandelion greens support compensatory secretions and can reduce post-meal sluggishness. These are gentle, food-based strategies that fit well within natural thyroid solutions and do not carry the risks of indiscriminate acid supplementation.
For B12, recent studies show that sublingual B12 can be as effective as intramuscular injections for many people. B12 injections are still a valid and fast option when neurological symptoms are present, but sublingual formulations are a convenient and effective alternative for ongoing maintenance.
Zinc and vitamin D repletion may be needed and should be guided by measured levels. Because thyroid medication absorption can be affected, discuss with your clinician whether changing formulation to a liquid or gel-cap form would help stabilize thyroid levels. That small change can make a big difference if gastric absorption is inconsistent.
When To Involve A Gastroenterologist And What Follow-up Looks Like
If the APCA test is positive but gastrin is normal, coordinate care with a clinician experienced in autoimmune endocrine and digestive conditions. Monitoring nutrient levels and treating deficiencies may be sufficient while you watch for progression. If gastrin becomes elevated or symptoms worsen, engage a gastroenterologist for endoscopy and mucosal assessment. Endoscopy allows for biopsy and early detection of precancerous changes, which is why it is recommended when gastrin suggests active mucosal damage.
Regular tracking matters. Recheck iron and ferritin after starting iron therapy, monitor B12 during repletion, and reassess gastrin periodically if initial results were concerning. Keep a record of symptoms such as new numbness, persistent heartburn, worsening fatigue, or changes in hair or skin because these can be early warning signs that deficiencies are progressing.
––Key takeaway: Screen with APCA/gastrin, address nutrient deficiencies, use mucin-supportive foods like cabbage, and favor digestive herbs and targeted nutrient replacement. Engage a gastroenterologist for follow-up and endoscopy if gastrin is elevated or symptoms worsen.
Practical Day-To-Day Steps That Help
Start by asking your clinician for an APCA test if you have Hashimoto’s disease and any of the symptoms discussed: unexplained fatigue despite thyroid optimization, early post-meal bloating, unexplained iron or B12 abnormalities, or neurological symptoms like numbness and tingling. If positive, expand testing to include gastrin and a full nutrient panel.
Adjust your diet to include mucilaginous and bitter foods daily. Try a simple routine of cabbage-based vegetable soup or a small serving of juiced cabbage mixed with apple before meals a few times a week. Add okra or squash into stews and roasted vegetable mixes. Use ginger, cumin, garlic, and turmeric throughout meals to boost digestive enzyme activity. Make bitter greens part of the salad rotation.
When supplementing, use targeted approaches. If iron is low, consider alternate-day dosing and take iron with vitamin C. If B12 is low, choose sublingual B12 if injections are not necessary or if you prefer a noninvasive option. Check zinc and vitamin D levels and replete as indicated. If your thyroid medication seems unpredictable, discuss liquid or gel-cap formulations with your prescriber to improve absorption.
Putting It Together: Prevention, Detection, And Effective Management
Start by asking your clinician for an APCA test if you have Hashimoto’s disease and any of the symptoms discussed: unexplained fatigue despite thyroid optimization, early post-meal bloating, unexplained iron or B12 abnormalities, or neurological symptoms like numbness and tingling. If positive, expand testing to include gastrin and a full nutrient panel.
Adjust your diet to include mucilaginous and bitter foods daily. Try a simple routine of cabbage-based vegetable soup or a small serving of juiced cabbage mixed with apple before meals a few times a week. Add okra or squash into stews and roasted vegetable mixes. Use ginger, cumin, garlic, and turmeric throughout meals to boost digestive enzyme activity. Make bitter greens part of the salad rotation.
When supplementing, use targeted approaches. If iron is low, consider alternate-day dosing and take iron with vitamin C. If B12 is low, choose sublingual B12 if injections are not necessary or if you prefer a noninvasive option. Check zinc and vitamin D levels and replete as indicated. If your thyroid medication seems unpredictable, discuss liquid or gel-cap formulations with your prescriber to improve absorption.
P.S. Whenever you are ready, here is how I can help you now:
- Schedule a Thyroid Second Opinion with me, Dr. C, Click Here for Details
- Need help to choose supplements? Click ‘Help Me Decide Here'
- Get my top books Here
Dr. Alan Glen Christianson (Dr. C) is a Naturopathic Endocrinologist and the author of The NY Times bestselling Hormone Healing Cookbook, The Metabolism Reset Diet, and The Thyroid Reset Diet.
Dr. C’s gift for figuring out what works has helped hundreds of thousands reverse thyroid disease, heal their adrenals, and lose weight naturally. Learn more about the surprising story that started his quest.



{kind=link}
{kind=link}